From injuries (bruises, dislocations and fractures) no one is insured. They happen as a result of strong overloads, falls, shocks. Today we will take a closer look at the types and ulna. Let's just say that such an injury does not happen too often. But a fracture of the ulna requires special attention, as it can impair the mobility of the arm.
What is a fracture?
A fracture is a violation of the integrity bone tissue part of the skeleton as a result of mechanical action, when the load on the bone exceeds its strength. It can be complete or partial, with or without displacement of bone processes. Sometimes they say that there is no fracture, just a crack. But this is a mistake! A crack is incomplete because its integrity is nevertheless broken.
Fractures are traumatic or pathological in nature. Traumatic injuries occur as a result of external influences, and pathological ones - as a result of the influence of painful deviations, for example, as a result of tuberculosis or a tumor.
The structure of the ulna
Elbow and articulated with each other and form the forearm. The bones run parallel. The body of the ulna is slightly longer. In addition, it has two ends with protruding processes: the ulna and coronoid (above) and the styloid (below). The processes are separated by a trochlear notch, to which the block of the bone of the shoulder adjoins. The olecranon of the ulna is a protruding place for attachment of the triceps and the coronoid process provides articulation of the ulna and radius. The styloid protrudes at the bottom of the bone and is easily palpable above the wrist. These are located between two joints:
- top - elbow;
- below - radiocarpal.
The ulna and radius are articulated in such a way that they provide pronation and supination of the forearm. Pronation is the ability to turn the forearm inward with the palm facing down. Supination is an outward rotation when the palm is turned up.
The structure of the ulna is very complex. can happen in any part.

ulna
The ulna is most often damaged in athletes, children and the elderly. The reasons are banal. Athletes subject the bones to severe overload, children are overly mobile, and their bones are not fully formed. Well, the old people are weakening in strength age features. Their bones more acutely feel the lack of calcium and become more fragile. Although with a lack of calcium, the risk of injury increases in all categories of people.
In medicine, several types of fracture of the ulnar bones have been distinguished:
- Damage to the olecranon. Usually the cause of such a fracture is trauma. This can be a fall on the elbow or a direct blow. The fracture may be oblique or transverse. Depending on the condition of the muscles, there may be different degrees process displacement.
- Fracture Malgenya. With such an injury, a process fracture and dislocation of the bones of the forearm occur. The hand takes a bent position, the palm is turned forward. The joint is enlarged and deformed. In addition to a traumatologist, a neurosurgeon or a pediatric neuropathologist should be invited (in case the child was injured).
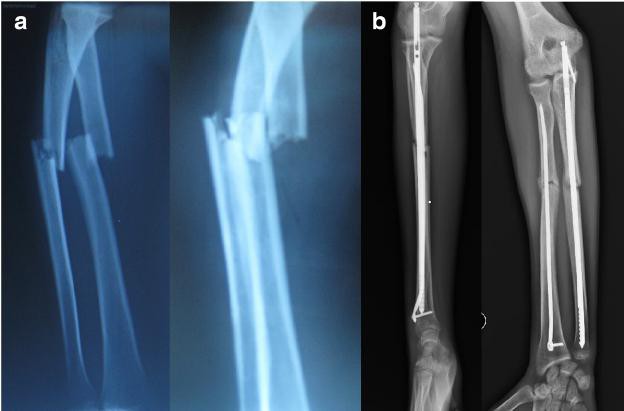
- Trauma in which dislocation of the head of the beam occurs. Another name is the Monteggia fracture. May be open or closed. The mobility of the joint is significantly limited. The forearm looks short on the injured side. In difficult cases, surgery is necessary. The ulna with a Monteggia fracture can be damaged in two types - flexion or extensor. The fixation option depends on the type of damage.
- Elbow fracture. One of the most common injuries. Movement in the joint is severely limited. Pain extends to the shoulder and forearm. Swelling is observed, bruising is formed.
- Fracture of the diaphysis. The diaphysis is the central part of the tubular bones. Debris displacement is rare. This is prevented by an intact radius. Hand deformity is observed.

General symptoms
The ulna, when damaged (fractured), looks somewhat deformed. The soft tissues around are swollen, movements are difficult and are accompanied by painful sensations. The symptoms of a fracture can vary, depending on the type of injury.
Fracture diagnosis
If dropped, hit, or violently jerked, causing severe pain, you need to see a traumatologist as soon as possible. A fracture of the ulna can have serious consequences. To prevent this from happening, it is important to get timely help.
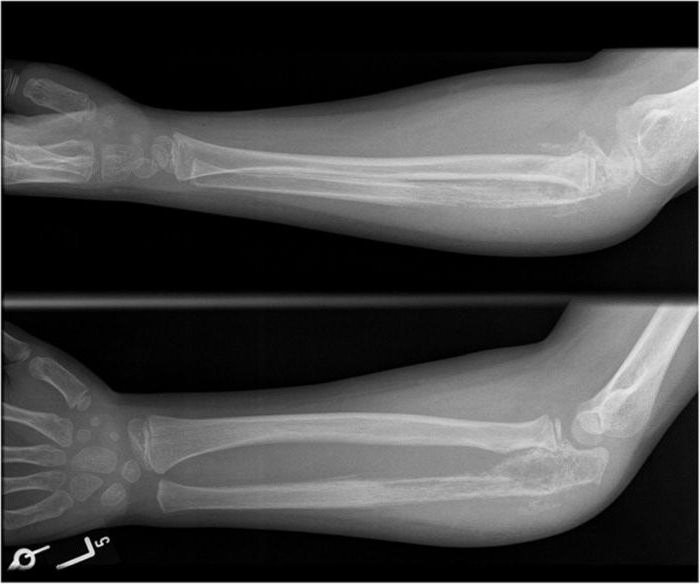
The traumatologist conducts a visual examination of the damaged limb and prescribes an x-ray. The doctor determines the type of fracture from the x-ray. In addition, he can consider whether the ulna is displaced at the site of injury. It depends on the treatment option for the fracture. In severe cases, the victim will need surgery.
Treatment
Diagnostics carried out by a traumatologist reveals the complexity of the problem. If a fracture of the ulna or bone elbow joint is not complicated by displacement, then a plaster cast is applied to the patient and a supporting bandage-kerchief is recommended. A week after the plaster is applied, a control x-ray is prescribed to make sure that no displacement has occurred. The plaster bandage is removed no earlier than after 3 weeks.
In case of displacement of bone fragments, the patient undergoes surgery. This may be a resection of the proximal fragment or the installation of a plate with screws to fix the injured bones. A plaster splint is used to immobilize the limb after surgery.
To restore mobility after a fracture, massages, physiotherapy and special exercises are prescribed.
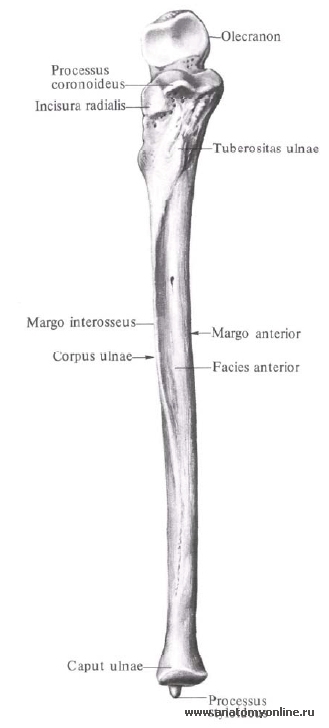
rice. 127 Upper limb bones ( ossa membri superioris) right; front view.Ulna, ulna (see Fig. , , , , , , ), long. It distinguishes the body and two epiphyses - proximal and distal.
Body of the ulna, corpus ulnae, trihedral shape. It has three edges: anterior (palmar), posterior (dorsal) and interosseous (outer) - and three surfaces: anterior (palmar), posterior (dorsal) and medial.
Anterior edge, margo anterior, rounded; rear edge, margo posterior, directed backwards, and interosseous margin, margo interosseus, pointed and turned towards the radius.
Anterior surface, facies anterior, somewhat concave. On it is nutrient hole, foramen nutricium, which leads to a proximally directed nutrient canal, canalis nutricius. In the upper part of the anterior surface, on the border between the body and the upper end of the bone, is located tuberosity of the ulna, tuberositas ulnae. Posterior surface, facies posterior, facing backwards, and medial surface, facies medialis, - towards the inner edge of the forearm.
Upper, or proximal, epiphysis, epiphysis proximalis, thickened, continues upward in olecranon. The anterior surface of this process is occupied block notch, incisura trochlearis, which is limited from below by the coronoid process, processus coronoideus. On the outer surface of the coronoid process is radial notch, incisura radialis, - the place of articulation of the ulna with the articular circumference of the head of the radius. Behind the radial notch begins arch support crest, crista m. supinatoris, which, following down, reaches the upper parts of the body of the bone.
 rice. 148 Bones of the forearm, right (X-ray). 1 - humerus; 2 - medial epicondyle; 3 - olecranon; 4 - ulna; 5 - styloid process of the ulna; 6 - lunate bone; 7 - navicular bone; 8 - styloid process of the radius; 9 - radius; 10 - tuberosity of the radius; 11 - neck of the radius; 12 - head of the radius; 13 - condyle head humerus; 14 - fossa of the olecranon..
rice. 148 Bones of the forearm, right (X-ray). 1 - humerus; 2 - medial epicondyle; 3 - olecranon; 4 - ulna; 5 - styloid process of the ulna; 6 - lunate bone; 7 - navicular bone; 8 - styloid process of the radius; 9 - radius; 10 - tuberosity of the radius; 11 - neck of the radius; 12 - head of the radius; 13 - condyle head humerus; 14 - fossa of the olecranon.. Lower, or distal, epiphysis, epiphysis distalis, the ulna is rounded. It distinguishes head of the ulna, caput ulnae. The surface of the head facing the wrist is smooth and concave. On the periphery of the head is located articular surface, – articular circumference, circumferentia articularis, ulna, articulating with radius. The medially posterior surface of the head continues into styloid process, processus styloideus; it is well felt through the skin.
Radius " src="http://i.enc-dic.com/dic/anatomy/images/aa/37_1.jpg">
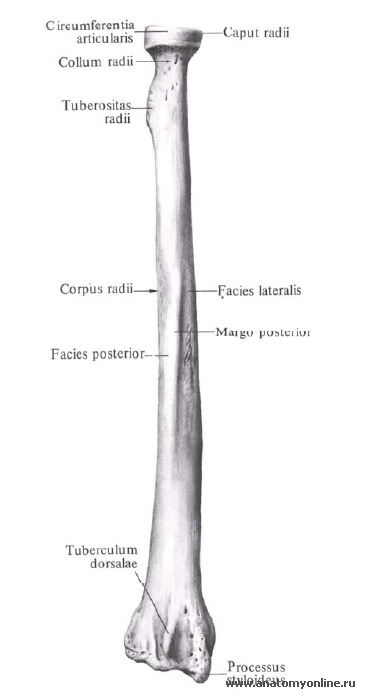
Radius, radius, is located outside and slightly anterior to the ulna. It distinguishes the body and two epiphyses - the upper and lower.
The body of the radius, corpus radii, is trihedral. It has three edges: anterior, posterior and interosseous (medial) - and three surfaces: anterior, posterior and lateral.
The anterior margin, margo anterior, and the posterior margin, margo posterior, are rounded.
The inner, or medial, edge of the bone is pointed, directed towards the ulna and is called the interosseous edge, margo interosseus.
The anterior surface, facies anterior, is somewhat concave. It has a nutrient hole, foramen nutricium, which begins the proximally directed nutrient channel, canalis nutricius.
The posterior surface, facies posterior, is smooth, separated from the lateral surface, facies lateralis, by the posterior margin.
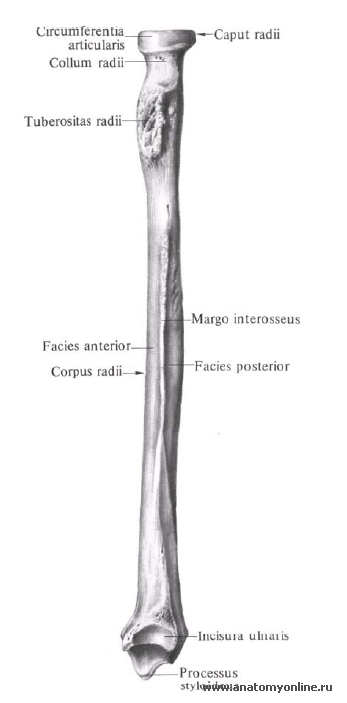
The upper, or proximal, epiphysis, epiphysis proximalis, on the border with the body bears a well-developed tuberosity of the radius, tuberositas radii, directed to the medial side. Above the tuberosity is a uniformly narrowed area of \u200b\u200bthe bone - the neck of the radius, collum radii. Above the neck is a cylindrical head of the radius, caput radii. Top surface the head is concave, it has an articular fossa, fovea articularis. The lateral part of the head carries the articular surface for articulation with the radial notch of the ulna and is called the articular circumference of the radius, circumferentia articularis radii (partially palpable through the skin).
The lower, or distal, epiphysis, epiphysis distalis, is thickened and expanded in the frontal plane. The styloid process of the radius, processus styloideus radii, departs from it, which is well palpable through the skin. On the inner surface of the lower end of the radius there is an ulnar notch, incisura ulnaris, which carries the articular surface for articulation with the articular semicircle of the head of the ulna. On the posterior surface of the distal epiphysis, closer to the styloid process, there is a dorsal tubercle, tuberculum dorsale, lying between the tendons m. extensoris policis longi and m. extensoris carpi radialis brevis.
The anterior surface of the lower epiphysis of the radius is smooth, on the back there are small ridges that separate the grooves in which the tendons of the muscles lie.
The lower surface is concave in the transverse and anteroposterior directions. It is the place of articulation with the bones of the wrist and is called the carpal articular surface, facies articularis carpea. It has a small scallop that runs in the anteroposterior direction and divides this surface into two parts, corresponding to the two bones of the wrist, which articulate with the radius at the wrist joint.
| Radius (radius). A-front view; B-back view. A: 1-carpal articular surface; 2-styloid process; 3-body of the radius; 4-front surface; 5-buffiness of the radius; 6-neck of the radius; 7-joint circumference; 8-head of the radius; 9-interosseous edge. B: 1-articular circumference (radius), 2-neck of the radius; 3-body of the radius; 4-interosseous edge; 5-back surface; 6-groove of the tendon of the long extensor muscle thumb brushes; 7-furrow of the mouse-radial extensor of the hand; 8-styloid process; 9-elbow tenderloin; 10-groove of the muscles - extensors of the fingers." align="left"> | Radius(radius). A-front view; B-back view. A: 1-carpal articular surface; B: 1-articular circumference (radius), |
Radius (lat. radius)- a paired bone of the forearm, located next to the ulna. It distinguishes the body and two ends: upper and lower.
 |
 |
 |
The body of the radius has a trihedral shape. Accordingly, there are three surfaces: front, back and side; and three edges: anterior, posterior, and interosseous. The anterior and posterior edges are rounded. The inner, edge of the bone is pointed, directed towards the ulna and is called the interosseous edge. Anterior surface slightly concave. It has a nutrient opening that continues into a proximally directed nutrient canal. The back surface is turned back, and the lateral surface is towards the outer edge of the forearm.
Atlas of human anatomy. Encyclopedias & Dictionaries. 2011 .
Free Part Skeleton upper limb
The skeleton of the free part of the upper limb (pars libera membri superioris) consists of the humerus (humerus), radius (radius) and ulna (ulna) bones of the forearm and bones of the hand (wrist bones, metacarpal bones and phalanges of the fingers).
Humerus (Fig. 25) - long tubular bone; its upper (proximal) spherical epiphysis, articulating with the glenoid cavity of the scapula, forms shoulder joint. The body of the humerus, cylindrical in its upper part, gradually becomes trihedral, ending with a wide, flattened in the anteroposterior direction of the distal epiphysis.
The upper epiphysis of the humerus, called the head of the humerus (caput himeri) (Fig. 25), is separated by a narrow interception - the anatomical neck (collum anatomicum) (Fig. 25) - from the large and small tubercles, separated by the intertubercular groove (sulcus intertubercularis) (Fig. 25). The large tubercle (tuberculum majus) (Fig. 25) lies in the lateral plane, and the small tubercle (tuberculum minus) (Fig. 25) is directed forward. The large and small tubercles are points of muscle attachment. The tendon of the biceps muscle of the shoulder passes through the intertubercular groove. A wide, smooth narrowing, located below the tubercles, as the weakest point of the humerus, most at risk of fracture, was called the surgical neck (collum chirurgicum) (Fig. 25).
A wide groove of the radial nerve (sulcus n. radialis) passes spirally along the body of the humerus (along the medial, with the transition to the posterior and lateral sides of the bone) (Fig. 25). On the lateral surface of the body of the humerus, closer to its upper epiphysis, there is a deltoid tuberosity (tuberositas deltoidea) (Fig. 25), to which the deltoid muscle is attached.
The lower epiphysis of the humerus has two articular surfaces, above which on both sides of the epiphysis are the lateral and medial epicondyles, which serve to attach the muscles of the forearm. The lateral articular surface, represented by the spherical head of the condyle (capitulun humeri), serves to articulate with the articular surface of the head of the radius. The medial articular surface has a cylindrical shape and is called the block of the humerus (trohlea humeri) (Fig. 25), the ulna articulates with it. Above the head of the condyle there is a radial fossa (fossa radialis) (Fig. 25), and above the block there are two fossae: coronal (fossa coronoidea) (Fig. 25) on the anterior surface of the bone and the olecranon fossa (fossa olecrani) (Fig. 25) on the back.
The bones of the forearm are represented by long tubular trihedral bones of the ulna and radius (Fig. 26, 27). These bones are in contact with their proximal and distal epiphyses, while their diaphyses are bent in opposite directions, forming the interosseous space of the forearm, filled with a strong fibrous interosseous membrane of the forearm (membrana interossea antebrachii).
The massive proximal epiphysis of the ulna has a block-shaped notch (incisura trochlearis) (Fig. 26, 28), the surface of which is covered with articular cartilage. The block-shaped notch is bounded from above by the olecranon (Fig. 26, 28), and from below by the coronoid process (processus coronoideus). The tuberosity located on the anterior surface of the bone below the coronoid process is called the tuberosity of the ulna (tuberositas ulnae) (Fig. 26, 28).
The superior and inferior epiphyses of the ulna articulate with the corresponding epiphyses of the radius. On the lateral side of the upper epiphysis of the ulna there is a radial notch (incisura radialis) (Fig. 26), the articular surface of which articulates with the head of the radius, forming the proximal radioulnar joint (articulatio radioulnaris proximalis). The lower epiphysis of the ulna - the head of the ulna (caput ulnae) (Fig. 28) - has an articular circumference (circumferentia articularis) (Fig. 26) for articulation with the ulnar notch of the radius. The posterior medial section of the distal epiphysis of the ulna ends styloid process(processus styloideus) (Fig. 26), the same process is present on the lateral side of the distal epiphysis of the radius.
The radius has a narrower proximal epiphysis; the head of the radius (caput radii) (Fig. 27) ends with the articular circumference (circumferentia articularis) (Fig. 27). Below the head of the radius, separated from it by the neck of the radius (collum radii) (Fig. 27), is the tuberosity of the radius (tuberositas radii) (Fig. 27). It serves to attach the biceps brachii.
The massive distal epiphysis of the radius articulates with its lower surface with the bones of the wrist. On the medial side of the distal epiphysis of the radius is the ulnar notch, through which the radius articulates with the ulna. The joints of the lower epiphyses of the ulna and radius form the distal radioulnar joint (articulatio radio-ulnaris distalis).
The wrist has the shape of a slightly curved groove, facing the bulge towards the back of the hand. The bones of the wrist (ossa carpi) are short, irregular in shape, arranged in two rows.
The proximal row is represented by the lunate (os linatum), scaphoid (os scaphoideum) and triquetral (os triquetrum) bones, as well as the pisiform bone (os pisiforme) adjacent to the triquetral bone from the palmar surface of the wrist. The distal row is made up of a trapezium bone (os trapezium), trapezoid (os trapezoideum), capitate (os capitatum) and hook-shaped (os hamatum) bones (Fig. 30). An elliptical bulge formed by the bones of the proximal row articulates with the distal epiphysis of the radius, and the bones of the distal row are connected with the bones of the metacarpus by a broken line of joints.
The metacarpal bones (ossa metacarpi) (Fig. 30, 36) are curved, facing the bulge towards the back of the hand. These bones are tubular; they distinguish between the base (basis metacarpalis), the body (corpus metacarpalis) and the head (caput metacarpalis). Connecting with the bases to the distal row of carpal bones, the metacarpal bones articulate with their heads with the bases of the phalanges.
The phalanges of the fingers (phalanges) (Fig. 30) also have a body, a base and a head. The bases of the proximal phalanges are connected to the heads metacarpal bones; the bases of the distal phalanges are connected to the heads of the proximal phalanges. In all fingers, except for the thumb, there are three phalanges (proximal, middle and distal), the thumb (I) finger has only two phalanges.