clavicle, is the only bone that holds the upper limb to the skeleton of the body. Its functional significance is great: it sets the shoulder joint at the proper distance from chest, causing greater freedom of movement of the limb. When comparing the clavicle various forms hominids, it can be seen that it gradually increases and in modern man becomes the most developed, which is associated with progressive labor activity. It is an integumentary bone that has moved on the body, therefore it ossifies partly on the soil of the connective tissue (its middle part), partly on the basis of cartilage (ends), while an independent ossification point is laid only on one (sternal) epiphysis (monoepiphyseal bone).
The clavicle ossifies both peri- and endochondral. The clavicle, according to the classification, belongs to mixed bones and is divided into a body and two ends - medial and lateral. The thickened medial, or sternal, end, extremitas sternalis, bears a saddle-shaped articular surface for articulation with the sternum. The lateral, or acromial, end, extremitas acromialis, has a flat articular surface - the place of articulation with the acromion of the scapula. On its lower surface there is a tubercle, tuberculum conoideum (trace of attachment of ligaments). The body of the clavicle is curved in such a way that its medial part, closest to the sternum, is convex anteriorly, and the lateral part is convex posteriorly.
Ossification. The clavicle receives an ossification point before all other bones - at the 6th week of intrauterine development. On the 16-18th year, a bone nucleus appears in the sternal end (pineal gland), which merges on the 20-25th year. Therefore, on radiographs of the girdle of the upper limb of people aged 16 to 25 years, at the sternal end of the clavicle, multiple islands of ossification can be found, which, merging, turn into a flat disk. In an adult, the anterior radiograph clearly shows the entire clavicle in a slightly S-shaped curve. On the lower surface of the clavicle, above the processus coracoideus of the scapula, a tuberculum conoideum is often seen, which can simulate inflammation of the periosteum in this area of the clavicle.
Which doctors to contact for examination of the Clavicle:
Traumatologist
What diseases are associated with the Clavicle:
What tests and diagnostics need to be done for the Clavicle:
chest x-ray
Are you worried about something? Do you want to know more detailed information about the Clavicle or do you need an examination? You can book an appointment with a doctor– clinic Eurolaboratory always at your service! The best doctors they will examine you, advise you, provide the necessary assistance and make a diagnosis. you also can call a doctor at home. Clinic Eurolaboratory open for you around the clock.
How to contact the clinic:
Phone of our clinic in Kyiv: (+38 044) 206-20-00 (multichannel). The secretary of the clinic will select a convenient day and hour for you to visit the doctor. Our coordinates and directions are indicated. Look in more detail about all the services of the clinic on her.
If you have previously performed any research, be sure to take their results to a consultation with a doctor. If the studies have not been completed, we will do everything necessary in our clinic or with our colleagues in other clinics.
You need to be very careful about your overall health. There are many diseases that at first do not manifest themselves in our body, but in the end it turns out that, unfortunately, it is too late to treat them. To do this, you just need to several times a year be examined by a doctor not only to prevent a terrible disease, but also to maintain a healthy spirit in the body and the body as a whole.
If you want to ask a doctor a question, use the online consultation section, perhaps you will find answers to your questions there and read self care tips. If you are interested in reviews about clinics and doctors, try to find the information you need on. Also register on the medical portal Eurolaboratory to be constantly up to date with the latest news and information updates about the Collarbone on the site, which will be automatically sent to you by mail.
Other anatomical terms starting with the letter "K":
| Brush |
| Foreskin (prepuce) |
| Clitoris |
| Knee-joint |
| Blood |
| Intestines |
| Blood vessels |
| telencephalon |
| Bone |
| Bone labyrinth |
| Cell |
| Adam's apple (Adam's apple) |
| blood capillaries |
| capillaries |
| Bone |
| Lower leg bones |
| Foot bones |
| coccygeal vertebrae |
| Coccyx |
| Sacrum |
| wrist bones |
| Knee |
Traumatic dislocations of the clavicle after dislocations of the shoulder and forearm take the third place. This frequency is due, on the one hand, to the anatomical and physiological characteristics of the clavicle joints, and, on the other hand, to the low susceptibility of its ends to complete intraarticular displacements, as a result of which subluxations occur more often in these joints than in others.
Anatomical and functional features of the clavicle
The clavicle is the only link between the upper limb and the trunk. The connection of the sternal end of the clavicle with the clavicular notch of the sternum formed the sternoclavicular joint, and the connection of the articular surfaces of the humeral end of the clavicle with the humeral process of the scapula formed the acromioclavicular joint. Both joints are simple. Their articular surfaces are covered with connective tissue cartilage, and in the acromioclavicular joint they are flat, beveled, elliptical in shape, in the sternoclavicular joint they are saddle-shaped. Their discrepancy is smoothed out by the articular disc, which is not always found in the acromioclavicular joint.
The acromioclavicular joint is surrounded by a dense fibrous capsule supported by strong ligaments (Fig. 16). One of them, acromioclavicular, is thrown between the humeral end of the clavicle and the humeral process of the scapula, the other, more durable, coracoclavicular, is stretched between the lower surface of the humeral end of the clavicle and the coracoid process of the scapula, which has cone-shaped and trapezoid parts. The joint is flat, multiaxial, but with a limited range of motion, which is carried out only in cooperation with the movements of the hand. It involves sliding of the clavicle in relation to the acromion, rotation of the scapula, as well as minor movements of the clavicle around its longitudinal axis.
 :
:
1 - acromion;
2-lig. acromioclaviculare;
3 - clavicula;
4-lig. coraclaviculare;
5 - scapula;
6 - processus coracoideus;
7-lig. coracoacromiale
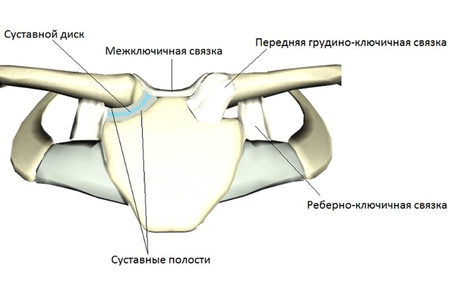
The sternoclavicular joint is enclosed in a wide, strong fibrous capsule, which is supported by three powerful ligaments. On the anterior, upper and posterior surfaces are the anterior and posterior sternoclavicular ligaments, the upper edge of the 1st rib with the clavicle is connected by the costoclavicular ligament, which inhibits the movement of the clavicle upward, and between the sternal ends of the clavicle over the jugular notch of the sternum handle, the interclavicular ligament is stretched. The latter inhibits the movement of the clavicle downwards. The sternoclavicular joint, being a two-chamber joint, approaches the spherical type in terms of range of motion. In it, movements are possible along all 3 mutually perpendicular axes of rotation, which, as a rule, are carried out in conjunction with the movements of the arm and shoulder blade (Fig. 17).

1-lig. interclaviculare;
2-lig. sternoclaviculare;
3 - clavicula;
4 - costa I;
5-lig. costaclaviculare;
6 - manubrium sterni
The clavicle performs the most extensive movements around the sagittal axis - up and down and around the vertical - forward and backward. If we take the center of rotation of the sternoclavicular joint as a fixed point, then the range of motion of the clavicle in all directions will be expressed at about 30-40 °, and its rotation around the longitudinal axis - at 20-25 °. Under the constant directing and regulating influence of the humeral end of the clavicle are the movements of the scapula, so the mechanical significance of the clavicle remains very important, since all the main biomechanical features shoulder girdle depend on the structure and function of the sternoclavicular joint. The area of the latter is completely not covered with muscles, and the clavicular-acromial joint is only covered in front by the deltoid muscle. At the same time, in the implementation of active movements, the muscles that attach to the collarbone are important. The sternocleidomastoid muscle and the sternoclavicular part of the large muscle approach the sternal end of the clavicle. chest muscle, and to the acromial end, in addition to the deltoid, the trapezoid approaches from above and behind. These active movements of the upper limb are impossible without the participation of the clavicle joints and the muscles attached to them; therefore, the shoulder, regardless of its initial position, cannot be raised above the horizontal. Along with the support ability of the shoulder girdle, the clavicle regulates the dynamics of the free upper limb, and also limits the convergence and dilution of the shoulder girdle.
Characteristics of dislocations of the clavicle
The percentage of dislocations of the clavicle to all dislocations in the joints of the extremities ranges from 2 to 17, and they occur mainly in middle-aged men. Depending on the degree of damage to the ligamentous apparatus, they can be complete and incomplete, and depending on the location, dislocations of the acromial end of the clavicle and sternal end are distinguished. The former are more common than the latter.
Atlas of traumatic dislocations. M.I. Sinilo, 1979
The sternoclavicular joint is one of the components of the bone girdle of the upper limb. Its role, along with the processes of the scapula and the ligaments surrounding them, is to create a strong framework for shoulder joint. But, given the high mobility in it, all these formations must be sufficiently flexible and plastic.
Thanks to these features, we can, for example, raise our arms above our heads in order to reach an object of interest. This is where their “double” purpose is manifested: on the one hand, they limit movement, and on the other hand, they protect the joint from excessive load.
Anatomical structure

From the name it is immediately clear that the sternoclavicular joint is formed by the corresponding bones. From the side of the arm, it is formed by the sternal segment of the clavicle, and from the chest - by the clavicular notch of the sternum. Various assumptions are made about the shape of this joint - it is stated that it is flat or spherical. These are wrong points of view, since the volume of movements is not suitable for a flat joint (too large), but for a spherical joint, the opposite is true.
- Simple - since it is formed by only 2 bones, enclosed in one common shell (capsule).
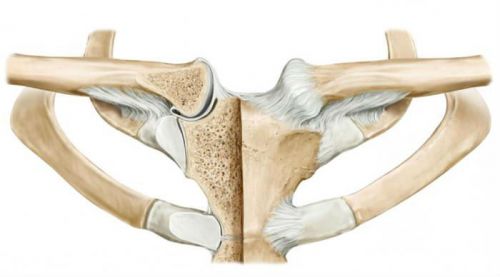
- The presence of an intra-articular disc gives it complexity. This is a thin plate of cartilage, which fuses with the capsule with its edges. This allows you to divide the articular cavity into two halves that do not communicate with each other.
- Saddle - means that the articular surfaces are S-shaped. The compound is arranged similarly in the body thumb hands. This gives sufficient mobility and flexibility combined with strength.
An interesting feature is that the clavicle is only one bone formation, which connects the hand to the human body.
Functions
For additional strengthening, the sternoclavicular joint is composed of four ligaments. They are insignificant in length and thickness, but cover it from all sides.
- From the front and back surfaces there are ligaments of the same name. They are wide and thin, can be woven into the joint capsule.
- Along the upper edges of the bones there is a common (for both joints) interclavicular fascia.
- The costoclavicular tendon is attached to the first rib from the lower surface of the clavicle. It is designed to create an additional fixation point to the chest.
Mobility in this joint is quite limited, but is performed in all planes (multi-axial connection).
Shrugging moves up and down. With their reduction and abduction - forward and backward, respectively. When rotating with your hands - the collarbones also make small circular movements.
Injuries of the sternoclavicular joint
Minor injuries to this joint, such as bruises and sprains, are rare. This is due to its small range of motion and protection from the possibility of a direct blow. Also important role plays the absence in it support function- the shoulder joint bears the main load.
Therefore, dislocations in this joint and fractures of the sternal end of the clavicle are most common. An important feature is a combination of these injuries with injuries to the arm and chest. Many important vessels and nerves pass under the clavicle, and even the slightest wound can lead to serious complications.
Dislocation

Their occurrence is always associated with indirect effects. This means that the damaging factor is the person's own weight. It is based on a fall on a straightened and tense arm laid back.
Most often this happens during ice or winter. The person suddenly falls and throws back the upper limb, trying to find support. A sharp blow is transmitted along the entire arm upward - to a reinforcing belt in the form of processes of the scapula and collarbone. Soft and thin ligaments cannot withstand such a load and are torn.
There are two variants of dislocation - anterior and posterior. They are distinguished depending on where the articular end of the clavicle has shifted - forward or behind the sternal notch.
Symptoms
External manifestations directly depend on the number of damaged formations. If only the joint capsule or internal disc is damaged, they may be minor. And if the surrounding ligaments were injured, then such an injury will be visible even to the naked eye.
- The first sign is a sharp pain, which will be determined at the junction of the collarbone with the sternum. Soreness and decreased mobility in the shoulder joint (inability to raise arms) will also be characteristic.
- Gradually, over several hours, swelling will increase in the clavicle area. This will lead to a change in the shape of the shoulder in the form of a shortening. pits all around clavicle(top and bottom) deepen sharply.
- When feeling in the region of the upper edge of the sternum, you can determine the dislocated end of the bone. If you press on the collarbone, then its mobility will appear, which is normally absent.
In terms of prognosis, posterior dislocation is much more dangerous - since there is a risk of injury internal organs neck (trachea, esophagus, blood vessels). Therefore, even if it is suspected, urgent help is needed.
To confirm the diagnosis, chest x-ray in two projections or computed tomography is used.
Conservative treatment

With the anterior variant, non-operative methods are almost always used. They include the following steps:
- They begin with anesthesia - they carry out a novocaine blockade or an anesthetic is injected intravenously.
- Then the patient is given a supine position, a roller is placed between the shoulder blades.
- After these procedures, traction is carried out for the injured arm, while simultaneously pressing on the protruding end of the clavicle.
- After reduction, a slight protrusion under the skin of the joint area is possible.
- The limb is immobilized for a month, using a plaster or soft bandage (such as Deso). Here the choice depends on the degree of damage to the ligamentous apparatus.
With the posterior view of the dislocation, all stages before the reduction technique are similar. Considering the nature of the displacement of the clavicle, when repositioning, they try to “pull” it back. Usually this is done with the help of fingers, clasping its end and pulling it towards you.
Restorative measures begin in a month and are performed within three weeks. They include therapeutic exercises and massage. Their goal is to normalize movements in the joint and strengthen muscles. Additionally, physiotherapy is prescribed in the form of warming procedures (UHF, electrophoresis, laser).
Surgery
Surgery is resorted to only in case of repeated ineffective reduction or a high risk of complications (posterior view). The use of metal structures (knitting needles) is strictly contraindicated. They can damage blood vessels and nerves that in large numbers pass under the collarbone.
The method of choice is suturing the articular end of the clavicle to the sternum. The surgeon sets the bone in place through a small incision and secures it with several sutures. The intervention is completed by strengthening the capsule and surrounding ligaments with the help of sutures and sections of their own tendons.
After the operation, a plaster cast is applied to the arm for a month. Then, for another 4 weeks, recovery is carried out. They start with passive exercises and massage, necessary for stretching the "new" ligaments. Then proceed to active physical education to strengthen them. Full recovery occurs after 2 months.
fracture

Most often occurs with a direct or tangential blow to the collarbone. Children usually suffer - their bones are still thin and fragile. And the great mobility and curiosity of the child lead to unplanned and awkward falls.
This injury may also be caused by a dislocation-like mechanism. With a sharp fall on a straightened arm or elbow, the blow is transferred to the collarbone and shoulder blade. Since the first is less durable, it breaks.
Symptoms
The signs are similar to dislocation, but are more pronounced and have a number of significant differences.
- Pain immediately occurs at the site of the fracture. Any attempt to move immediately causes discomfort. Therefore, the person holds the injured hand by the forearm and presses it to the body.
- Swelling occurs around the clavicle, a hemorrhage is determined at the site of the fracture under the skin.
- The shoulder moves forward and down, its width is less than that of a healthy one.
- At the site of the sternal end of the clavicle, a retraction is determined. This is due to the upward displacement of the fragment under the action of the muscles.
Confirm the diagnosis with an x-ray. The picture clearly shows the line of fracture and displacement of fragments. Do not forget about the risk of injury to blood vessels and nerves by bone fragments. Therefore, while moving to the hospital, it is necessary to immobilize the limb with improvised means (a wooden splint or a bandage-kerchief).
Conservative treatment

It is used only for uncomplicated fractures. Insufficient comparison of fragments is not an indication for surgery, since in the future, under the action of the muscles, the clavicle will acquire a normal shape.
- They start with anesthesia - they perform a novocaine blockade or inject an anesthetic directly into the hemorrhage.
- Then, relaxation of the muscles pulling the fragments is performed. To do this, the shoulder blades are reduced as much as possible and the head is tilted to the side (in the direction of the fracture).
- After that, the surgeon, using pressure on the bone, returns the fragments to their usual place and holds them.
- In this position, a plaster cast is applied to the arm for a month and a half. It has a special structure and consists of 2 separate bands (according to Weinstein). This allows you to freely perform x-rays and restorative measures.
Physiotherapy methods have been used since 2 weeks. They include procedures that improve local blood flow (UHF, electrophoresis, massage). After removing the bandage, they begin to do physiotherapy exercises to strengthen the muscles (at least 2 months).
Surgical treatment

Surgery is performed only if there is a high risk of complications. Such situations occur with a strong displacement of fragments and the impossibility of their reduction. This can lead to damage to blood vessels, nerves or internal organs (lung).
In such cases, an operation is performed, during which the broken ends of the clavicle are fixed with a special plate. After the intervention, the hand is immobilized with a soft bandage for three weeks. The metal structure is removed after a year.
Currently, the early recovery technique is being used. Physiotherapy and therapeutic exercises begin 2 days after the operation. Their appointment is shown for a period of at least 3 months.
How to forget about pain in the joints?
- Joint pain limits your movement and life...
- You are worried about discomfort, crunching and systematic pain ...
- Perhaps you have tried a bunch of medicines, creams and ointments ...
- But judging by the fact that you are reading these lines, they did not help you much ...
But orthopedist Sergei Bubnovsky claims that indeed effective remedy for joint pain exists!
The sternoclavicular joint is one of the main joints of the upper limb girdle, which creates a strong and reliable frame for the shoulder joint, which attaches the human arm to the chest. Despite the high strength of the articulation, it is also very flexible, which allows the collarbone, and with it the entire upper limb, to move in three different planes.
Thanks to this joint, a person can raise his arms up, put them behind his head, and perform rotational movements in his shoulders. If the function of the sternoclavicular joint suffers due to injury or disease, then full range of motion in the shoulder joint becomes impossible.
The sternoclavicular joint has, as it were, a double meaning. On the one hand, it limits mobility in the girdle of the upper limb, ensuring its stability, and on the other hand, it helps the hand to perform high-amplitude movements.
Articulation Anatomy
The sternoclavicular joint is formed by the clavicular notch on the sternum and the sternal end of the clavicle. The articular surfaces of the bones are covered with hyaline cartilage, which does not provide complete congruence.
For reference: the congruence of the joint is the complete mutual correspondence of the shape of the articular surfaces of the bones that articulate with each other. If the surface of the joint loses its congruence, then movements become difficult, and in some cases impossible.
But nature took care of man and found an excellent solution to such a problem. As for the sternoclavicular joint, the issue of complete congruence is resolved with the help of an intra-articular disc, which is located between articular surfaces two bones without articulating with them. It is attached around the perimeter to the joint capsule. This disk divides the articular cavity into 2 separate parts: lower middle and upper lateral. In some people, the intra-articular disc may have a hole in the middle and both articular cavities in such cases are interconnected.
What does the sternoclavicular joint look like?
There are still discussions among anatomists about the classification of this articulation. Some experts argue that the joint is flat, others insist that it is spherical in function, others classify it as saddle. Since the amplitude of movements is too large for a flat joint, and, on the contrary, too low for a spherical joint, we will assume that the sternoclavicular joint is saddle-shaped, simple and complex in structure.
A simple joint is one that is formed by no more than two articular surfaces of bones.
Complex joint- this is one that contains additional cartilage components inside the joint capsule to ensure congruence. In this case, it is an intra-articular cartilage disc.
saddle joint- this is the one that is formed by 2 articular surfaces, which, as it were, sit astride each other. In this case, the movements are carried out by sliding one bone along the other. This provides mobility in two mutually perpendicular axes. But, as it was said, movements in the sternoclavicular joint are possible in 3 planes (there is also a small amplitude rotation of the sternal end of the clavicle), which became the reason for the disputes of scientists. But, according to the opinion of the majority, this articulation is still considered a saddle.
From above, the joint is covered with a dense capsule and sealed with several very strong ligaments:
- The sternoclavicular ligament (anterior and posterior), which reinforce the articulation capsule along the anterior, superior, and posterior surfaces. They are wide, but short, and can be woven into the connective tissue of the capsule along their length.
- The costoclavicular ligament originates from the upper edge of the first rib and attaches to the clavicle. It is very dense, wide and strong. It inhibits increased mobility in the joint upwards and stabilizes the belt of the upper limb.
- The interclavicular ligament is stretched between the two sternal ends of the clavicle above the jugular notch of the sternum. It limits unnecessary downward mobility of the collarbone.
Joint functions
The anatomical features of the structure of the sternoclavicular joint allow movement in it in three planes:
- around the vertical axis (reduction and dilution of the shoulders and shoulder blades);
- around the sagittal axis (raising and lowering the shoulders);
- around the frontal axis (rotational movements in the shoulders).
Also, the sternoclavicular joint is the only articulation that connects axial skeleton a man with an upper limb. It is worth noting that in humans, this joint is to some extent rudimentary, that is, one that has lost its functional purpose in the process of evolution and upright walking. In animals, it performs much more functions, and the amplitude of movements in it is very large.
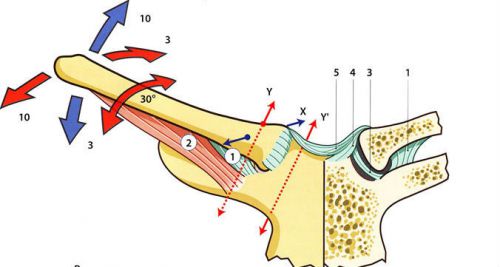
The diagram shows the amplitude of possible movements in the joint
Articulation assessment methods
In this pairing, all types of movements are combined with those in the acromioclavicular and shoulder joints. His condition can be assessed by examination, palpation and additional research methods (X-ray, MRI, CT).
Inspection
When visually inspecting the joint, it is not always possible to clearly see it, since well-developed subcutaneous fatty tissue can interfere with this. In people with overweight, the joints are not visible, but in people with an asthenic physique (in thin people), the joint is clearly contoured. Helps to identify the articulation of the rise of the shoulders. Normally, both sternoclavicular joints are symmetrical, the skin color above them is not changed, there is no swelling, movements are free, painless and not accompanied by crepitus (crunching).
In case of detection of deformation of skin hyperemia over the joint, pain or limitation of amplitude during movements, edema, any pathology (disease or injury) should be suspected.

In thin people, the sternoclavicular joint is clearly visible and accessible for visual inspection. In this image, you can clearly see the deformation of the left joint
Palpation
The palpation of the joint is carried out by the doctor with the 2nd and 3rd fingers of one hand. To improve the quality of palpation, it is necessary to raise the shoulders and bring the joints into an advantageous position for examination. To better assess mobility, the patient is asked to move their shoulders back. In this case, the capsule is stretched in front.
Normally, the joint is not painful to the touch, there is no edema and an increase in local skin temperature, there is no crepitus or deformity, the range of motion is within normal values.
From additional methods researches use most often a roentgenography of a thorax. In severe cases, MRI or computed tomography may be required for diagnosis.

Radiography and CT scan allow a good study of the structure of the joint and identify possible damage
Possible diseases
As already mentioned, any lesions of this joint affect the possibility of free movements of the upper limb and significantly reduce the quality of life of such patients. Any daily activity they have is accompanied by pain and the inability to perform the desired movement. Consider the most common types of diseases of the sternoclavicular joint.
Arthrosis
Arthrosis of this joint is one of the rare and little-known localizations of this disease. Most often, it occurs after an injury and is unilateral in nature; it is very rare to find simultaneous damage to both joints.
Most often, this disease occurs under the guise of humeroscapular periarthritis, arthrosis of the shoulder joint, intercostal neuralgia, osteochondrosis, and angina pectoris. Very often, such patients are misdiagnosed, which leads to prolonged and unsuccessful treatment.
The following signs will help in the diagnosis:
- pain when feeling the area of the sternoclavicular joints;
- development of deformity in this part of the body;
- mild swelling;
- the presence of a crunch when moving;
- discomfort and pain when lying on the stomach.
X-ray of the joint area helps in the diagnosis, where pathological changes typical of arthrosis are detected.
This disease responds well to treatment. Apply physical therapy, manual therapy, physiotherapy, medications for elimination acute pain. If necessary, perform a blockade of the connection area with glucocorticosteroid drugs.
Arthritis
This is an inflammation of the sternoclavicular joint, which can have several causes. Most often, this joint is affected in reactive polyarthritis (Reiter's syndrome). Acute purulent arthritis can also develop when an infection enters the joint cavity. In some cases, this compound can be drawn into the pathological process during systemic autoimmune diseases, for example, with rheumatoid arthritis, Bechterew's disease, etc.
Arthritis symptoms:
- acute pain in the joint area, which increases with any movement;
- swelling and redness of the skin over the joint, increased local temperature;
- inability to freely move the arm due to pain;
- common signs: fever, malaise, muscle pain, weakness.

This is what sternoclavicular arthritis looks like
Treatment for arthritis of the sternoclavicular joint depends on its cause. Therefore, when these signs appear, it is necessary to seek help from a therapist, orthopedist or rheumatologist. If arthrosis is not treated, then ankylosis of the joint may occur, that is, the complete disappearance of the articular cavity and immobility. And this condition can be corrected only through surgical treatment.
Injuries
Most often, one has to deal with a dislocation in the sternoclavicular joint, with a partial or complete rupture of its ligaments.
The development of such an injury is associated with a direct damaging effect in this area, for example, with a blow or a fall on a straightened arm laid back.
Two variants of dislocation are possible: anterior and posterior (depending on where exactly the sternal end of the sternum has shifted - to the anterior or posterior part of the sternum).
The following symptoms may help to suspect a dislocation:
- sharp pain at the site of injury, which increases with any movement;
- increasing edema, deformation of this anatomical zone, bruising, hematoma;
- on palpation, you can feel the displaced end of the clavicle;
- a significant limitation of active movement of the hand and a sharp pain when trying to passive movements;
- when pressing on the clavicle, you can detect increased mobility of the bone, which is normally absent.
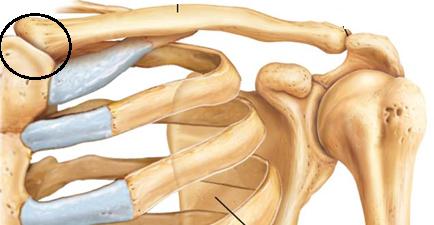
![]()
Anterior dislocation with displacement of the sternal end of the clavicle to the anterior surface of the sternum
When there is a danger of injury to the organs of the neck and chest, so the patient should be immediately taken to a trauma hospital, where he will be provided with all the necessary assistance.
Depending on the type of damage and its degree, treatment can be conservative or surgical.
There are also rarer diseases of the sternoclavicular joint, for example, Friedrich's syndrome (aseptic necrosis of the sternal head of the clavicle), SAPHO syndrome (a combination of hyperostosis of the sternoclavicular joint with pustular lesions of the palms and soles, psoriasis or acne, spinal lesions in the form of osteitis, arthritis, sacroiliitis), but they occur in isolated cases.
Thus, the sternoclavicular joint is a small but very important joint in our body. A violation of the function of this joint leads to the inability to perform hand movements, to significant discomfort, disability and a decrease in the quality of life of such patients.
The sternoclavicular joint is not always clearly visible. It usually manifests itself in people who are underweight or asthenics. If there is a small amount of subcutaneous adipose tissue, it can be considered. In people with normal or increased body weight, it is visually indistinguishable. On palpation, they are guided by the clavicle bones, between which, at the junction with the sternum, below the cervical fossa, there are two symmetrical sternoclavicular joints.
Definition and location of the joint
sternoclavicular joint - this is the junction of the clavicle with the sternum. It has an asymmetrical shape, which allows you to compensate for the difference in size and shape of the bone notch and collarbone, allowing them to perfectly match each other. Inside the joint is the articular disc, which compensates for the pressure between the bones, being a connecting element. From above, the entire joint is covered with cartilaginous tissue, which protects it from external influences and damage.
The sternoclavicular joint. Characteristic
The purpose of the joint is to connect upper limbs with the chest by combining the bones of the clavicle and shoulder girdle with the body. In origin, the sternoclavicular joint - this is a rudiment, which is a connection of the upper or forelimbs, not only in humans, but also in animals, starting with reptiles. It is very strong and participates in the movement of the hands, the reformation. This is especially felt when raising your hands up and down. This connection allows the clavicle to move along three main axes, synchronizing with a powerful and very strong ligamentous apparatus supported.
Structure
The sternoclavicular joint is shaped like a saddle joint. According to its structure, it has a communicating shape, having concavities and convexities corresponding to each other. This joint, having two axes and freely moving along them, from the point of view of simple mechanics, is a universal joint. Its structure includes such cartilaginous tissues:
- cartilaginous covering of the clavicle;
- cartilaginous covering of the sternocostal cavity;
- cartilage disc;
- cartilage covering the joint.

Thus, the structure of the joint includes:
- the medial end of the clavicle with its main surface;
- ligament upper;
- ligament anterior;
- costoclavicular ligament;
- posterior ligament;
- concave arches of the sternocostal surface.
The sternoclavicular joint is also supported by:
- Intervertebral ligament, stretching over the notch of the jugular cavity of the sternum between the ends of the clavicular bones.
- The sternoclavicular ligament complex. According to their location, they converge on the front, back and upper surfaces joint, strengthening its strength.
- The most powerful and durable ligament in the sternum is the costoclavicular. It runs from the very top edge at the first rib and rises to the collarbone. Controls the maximum lifting of the clavicle up.
The sternoclavicular joint, having a saddle-shaped structure in shape, resembles spherical ones in terms of the possibilities of its movement.
Damage
Due to its superficial location and role in movement between the bones and joints of the shoulder girdle and trunk, the clavicle itself and the joints attached to it are often subject to fractures and dislocations. Dislocation occurs as a result of sharp movements of the shoulder girdle backwards or downwards and backwards. In this case, the anterior ligament is torn, forming a subluxation. With a stronger impact on this joint, all ligaments are torn, releasing the clavicle from the articular fossa, forming a dislocation of this joint, which is easily recognized by external signs. Another type of dislocation occurs if the impact on the collarbone and joint is direct, that is, by a direct blow or strong pressure when the posterior ligament is torn. Such a dislocation occurs inside. It also occurs when the joint is affected by a strong compression of the shoulders forward and inward. As a rule, under such influences, a fracture of the first or first four ribs of the sternum is also observed.
Diseases
This joint is characterized by diseases such as ankylosis, which is a consequence of gonococcal or rheumatoid arthritis. After the age of forty, arthrosis often appears, which during its course forms marginal osteophytes on the head of the clavicle. Soreness caused by exposure to sternoclavicular swelling should be the reason for a visit to an osteopath.

The end of the clavicle attached to the sternum, which is better known as determined by palpation. Causes painful swelling of tissues around the joint, swelling and redness skin. Hyperostotic changes in the attached end of the clavicle are manifested in (Paget's disease). The manifestation of hyperostosis is typical of congenital syphilis.
Diagnosis of changes in the joint
Methods for diagnosing diseases and disorders in the sternoclavicular joint are examination and palpation, X-ray of the bones of the chest. All studies are carried out by a traumatologist or osteopath. Any asymmetry or deformity, redness or pain when moving in the sternoclavicular joint, the appearance of a crunch in movement indicates the presence of one of the above diseases or injuries.

Palpation is carried out with the second and third fingers right hand, while the doctor is located behind or to the side of the patient. The fingers are placed in the middle of the sternum and, focusing on the notch under the patient's neck, feel for the joint. For better detection of his patient, they are asked to raise their hands in a horizontal plane, which greatly facilitates the search.
The sternoclavicular joint is simple in structure. But at the same time, he is quite strong, keeps the limbs attached to the body. With damage to this joint, the movements of the hand become very limited and bring pain.